
Manual vs Digital Blood Pressure Monitors - Which Is Right for You?
.png)
Manual blood pressure monitors offer greater clinical precision; digital monitors offer speed and consistency. The right choice depends on your setting: trained clinicians often prefer manual (aneroid) devices for complex cases, while digital monitors suit home users and high-volume screening. Most clinical guidelines recommend using both, digital for routine measurement, manual for confirmation.
This guide breaks down accuracy, ease of use, cost, and the best devices for each setting so you can choose with confidence.
TL;DR
Quick Summary: Manual vs. Digital Blood Pressure Monitors
| Manual (Aneroid) | Digital | |
|
Accuracy |
±3 mmHg (operator-dependent) | ±3 mmHg (automated) |
|
Best for |
Clinical confirmation, EMS, training | Home use, screening, busy clinics |
|
Ease of use |
Requires training | Minimal training needed |
|
Power needed |
No | Yes (battery/charging) |
|
Cost |
Lower upfront | Higher upfront |
|
Irregular rhythms |
Better detection | Algorithm limitations |
Bottom line: Use digital for speed and consistency. Use manual when accuracy is critical or patient factors complicate automated readings.
How Manual Blood Pressure Measurement Works
Manual blood pressure monitors, also known as aneroid sphygmomanometers, use an inflatable cuff, pressure gauge, and the stethoscope to measure blood pressure through auscultation.
This method remains a clinical standard because it allows trained users to directly hear arterial sounds and control the measurement process.
Entry-level tools like the ADC Basic Aneroid Sphygmomanometer (450-776Z) provide a reliable starting point, featuring:
- A precision-calibrated manometer gauge
- Index and range markings to support proper cuff placement
- A compact, pocket-sized design for portability
 For clinicians needing greater durability and long-term performance, the ADC Prosphyg ™ 760 Pocket Aneroid (401-760-11ABK) offers:
For clinicians needing greater durability and long-term performance, the ADC Prosphyg ™ 760 Pocket Aneroid (401-760-11ABK) offers:
- ±3 mmHg accuracy across standard temperature ranges
- A 300 mmHg black enamel manometer built for daily use
- ADC’s Size Guide™ cuff system, helping prevent mis-cuffing errors
 Together, these tools illustrate how manual monitors can scale from student use to professional clinical environments.
Together, these tools illustrate how manual monitors can scale from student use to professional clinical environments.
The Case for Aneroid Sphygmomanometers
Manual devices continue to be preferred in many healthcare environments for several reasons:
High Accuracy with Proper Technique
Manual monitors provide clinically validated accuracy (typically ±3 mmHg) when used correctly, especially in controlled clinical environments.
Durability and Long-Term Reliability
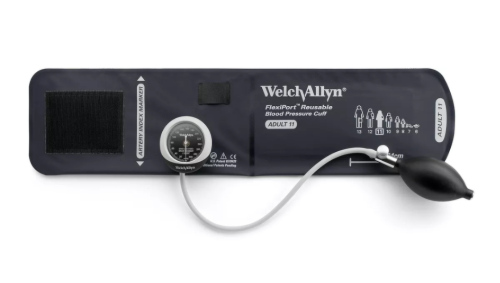
Professional-grade models such as the Welch Allyn DuraShock ™ DS45 (450-DS45.11) are engineered for long-term reliability, featuring:
- Certified accuracy of ±3 mmHg
- Gear-free DuraShock™ technology, helping maintain calibration longer than traditional designs
- 30-inch drop resistance, meeting AAMI shock standards
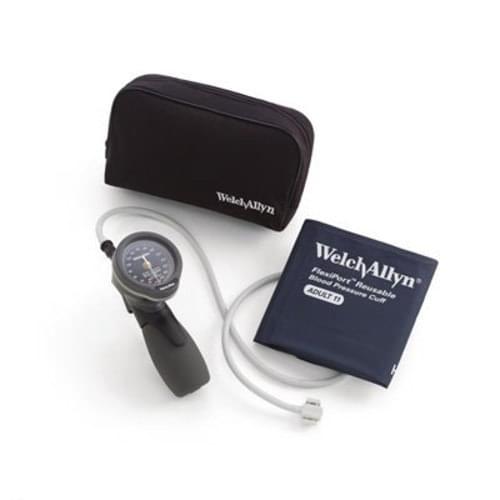
 For clinics requiring flexibility across multiple patient types, the DS45 Multi-Cuff Kit (450-DS45MC) includes:
For clinics requiring flexibility across multiple patient types, the DS45 Multi-Cuff Kit (450-DS45MC) includes:
- Four FlexiPort® cuffs (child to large adult)
- Quick cuff changes with a single-point connection system
 In high-demand environments, advanced options like the Welch Allyn Gold Series DS66 Trigger Aneroid with 4 Cuff Kit (450-5098-30) and Welch Allyn Tycos Gold Series DuraShock DS66 Hand Aneroid with Adult Cuff (FlexiPort) (450-5098.27) add:
In high-demand environments, advanced options like the Welch Allyn Gold Series DS66 Trigger Aneroid with 4 Cuff Kit (450-5098-30) and Welch Allyn Tycos Gold Series DuraShock DS66 Hand Aneroid with Adult Cuff (FlexiPort) (450-5098.27) add:
- One-handed trigger deflation control for precision
- Jeweled movement mechanisms for extended instrument life
- Up to 15-year calibration warranties
These features make them ideal for high-volume clinics, family practic, and long-term clinical use.

No Power Required
Manual monitors operate without batteries or charging, making them ideal for:
- Mobile clinicians
- Emergency response
- Training environments
Greater Clinical Control
Clinicians can control inflation, deflation, and auscultation technique, especially important for complex or irregular readings.
The Case for Digital Blood Pressure Monitors
Digital blood pressure monitors automate the measurement process, providing fast and easy readings with minimal training required.
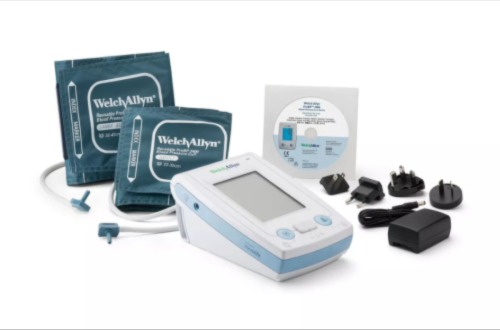
A leading example is the Welch Allyn ProBP ™ 2400 Digital Blood Pressure Device (100-2400), designed for modern clinical workflows.
This device combines automation with advanced diagnostic support, including:
- ±3 mmHg measurement accuracy
- Three-reading averaging mode to improve diagnostic reliability
- Irregular heartbeat detection for added clinician insight
- Microprocessor-controlled deflation, reducing user error
Measurement range:
- Systolic: 60-255 mmHg
- Diastolic: 30-200 mmHg
The ProBP 2400 supports a wide range of patient needs while delivering consistent, repeatable readings across users.
Ease of Use
Digital devices are simple to operate, making them ideal for:
- Home users managing hypertension
- Busy clinics with multiple staff members
- Screening environments
Consistent Measurement Technique
Automated inflation and deflation reduce user variability, improving consistency across readings.
Advanced Clinical Features
Modern digital monitors often include:
- Multi-reading averaging
- Irregular heartbeat detection
- Controlled deflation technology
These features help provide a more complete picture of patient cardiovascular health.
Improved Workflow Efficiency
Digital devices support faster patient throughput, making them valuable in high-volume settings.
Accuracy Comparison: Manual vs. Digital Blood Pressure Monitors
Both device types can achieve clinically validated accuracy of ±3 mmHg — the benchmark set by AAMI standards — but how they get there differs significantly.
Manual (Aneroid) Monitors
Manual devices measure blood pressure through auscultation: a trained user listens for Korotkoff sounds while controlling cuff inflation and deflation. Accuracy depends heavily on the operator.
Strengths:
- ±3 mmHg accuracy when used by trained clinicians
- Less affected by irregular heart rhythms (atrial fibrillation, arrhythmias)
- Allows detection of subtle arterial sounds digital algorithms may miss
- No algorithmic interpretation — the clinician hears and decides
Limitations:
- Accuracy is operator-dependent; errors increase with less experienced users
- Requires proper cuff placement, controlled deflation rate, and quiet environment
- Not practical for self-measurement at home
When manual is the better choice: Patients with arrhythmias, severe obesity, advanced arteriosclerosis, diabetes affecting circulation, or weak pulse signals — situations where automated algorithms are more likely to produce unreliable readings.
Digital (Automated) Monitors
Digital monitors use oscillometric technology, detecting arterial wall vibrations rather than sound. A microprocessor interprets these oscillations to calculate systolic and diastolic pressure.
Strengths:
- ±3 mmHg accuracy; ±5% pulse accuracy (e.g., Welch Allyn ProBP 2400)
- Eliminates operator variability — same technique every time
- Three-reading averaging modes improve diagnostic reliability
- Irregular heartbeat detection flags readings that may need follow-up
- Faster workflow in high-volume settings
Limitations:
- Algorithms may underperform in certain patient populations
- Requires power source (batteries or charging)
- Higher upfront cost
When digital is the better choice: Routine screening, home monitoring, high-volume clinics, or any setting where consistent technique across multiple users matters more than nuanced clinical control.
Head-to-Head: The Honest Answer
Neither device type is universally superior. Clinical best practice — supported by major cardiovascular health organizations — increasingly recommends a combined approach:
- Digital for initial screening and routine monitoring
- Manual for confirmation when readings are abnormal, borderline, or the patient has factors that reduce digital accuracy
Regardless of device type, cuff fit remains the single biggest accuracy variable. An incorrectly sized cuff can shift readings by 5–10 mmHg, more than the difference between most comparable devices.
What the Research Says
Clinical evidence supports using both device types strategically:
- The American Heart Association (AHA) recommends upper-arm automated devices for home blood pressure monitoring, noting they reduce measurement error compared to manual technique in unsupervised settings.
- A 2019 review in Hypertension found that automated office blood pressure measurement (AOBP) produces readings closer to ambulatory blood pressure than traditional manual auscultation, due to the elimination of white-coat effect during attended measurement.
- AAMI/ISO standards (the benchmark for device certification) require blood pressure monitors to achieve a mean error of ≤5 mmHg with a standard deviation ≤8 mmHg, both manual and digital devices in this guide meet or exceed that threshold.
- Studies consistently show that cuff sizing errors account for a larger share of measurement inaccuracy than device type, underscoring the importance of proper fit regardless of which monitor you choose.
Sources: American Heart Association, Hypertension (AHA Journal), Association for the Advancement of Medical Instrumentation (AAMI)
Cost, Maintenance, and Longevity
Manual Monitors
- Lower upfront cost
- Minimal maintenance
- Long lifespan
- Occasional calibration checks required
Digital Monitors
- Higher initial investment
- Require batteries or charging
- More components that may require servicing
In high-use environments, manual monitors are often more cost-effective long-term.
Choosing the Right Blood Pressure Monitor for Your Setting
The best blood pressure monitor depends on where it’s being used and who is using it.
Different settings prioritize different things —accuracy, speed, ease of use, or portability.
Use the guide below to quickly find the right fit.
Clinical Settings (Clinics, Hospitals, Outpatient Care)
Best for: Accuracy + efficiency in high-volume environments
What matters most:
- Fast patient throughput
- Consistent readings across staff
- Ability to confirm results when needed
Recommended Setup:
- Digital for screening + manual for confirmation
Top Picks:
- Manual: Welch Allyn DuraShock DS45
- Multi-patient use: Welch Allyn DS45 Multi-Cuff Kit
- Advanced control: Welch Allyn DS66 Trigger Aneroid
Why this works:
- Digital improves workflow speed
- Manual ensures clinical accuracy when readings are uncertain
Home Use (Patients & Caregivers)
Best for: Simplicity + consistency
What matters most:
- Easy operation
- Reliable readings without training
- Clear, repeatable results
Top Picks:
- Easy, automated: Welch Allyn ProBP 2400 Digital Blood Pressure Device
- Budget manual option: ADC Basic Aneroid Sphygmomanometer
Why this works:
- Digital devices remove user error
- Manual devices are viable if the user has training
EMS & Mobile Care (Field Use, Home Visits, First Responders)
Best for: Reliability + portability
What matters most:
- No reliance on power or batteries
- Durability in unpredictable environments
- Fast, dependable readings
Top Picks:
- Portable professional: ADC Prosphyg 760 Pocket Aneroid
- Premium durability: Welch Allyn Gold Series DS66 Hand Aneroid
Why this works:
- Manual devices function anywhere
- Compact designed fit mobile workflows
Training & Education (Students & Clinical Training Programs)
Best for: Skill development + foundational learning
What matters most:
- Learning proper technique
- Understanding auscultation
- Building clinical confidence
Top Picks:
- Beginner-friendly: ADC Basic Aneroid Sphygmomanometer
- Step-up option: ADC Prosphyg 760 Pocket Aneroid
Why this works:
- Manual devices teach core clinical skills
- Builds a foundation before using digital tools
Quick Decision Guide
| Setting | Best Choice |
|
Clinical |
Digital + Manual |
|
Home |
Digital |
|
EMS / Mobile |
Manual |
|
Training |
Manual |
Why Cuff Size Matters More Than the Device
Choosing the right monitor is important, but cuff size has an even greater impact on accuracy.
Incorrect cuff sizing can lead to:
- Too small → falsely high readings
- Too large → falsely low readings
Multi-cuff systems such as the Welch Allyn DS45 Multi-Cuff Kit (450-DS45MC) ensure accurate readings across a wide range of patients, especially in clinical settings.
Final Thoughts
Manual and digital blood pressure monitors are not competing tools, they are complementary.
- Manual devices provide precision and control
- Digital devices offer speed and consistency
The best choice ultimately depends on your environment, experience level, and clinical needs.
Frequently Asked Questions
Are manual blood pressure monitors more accurate than digital? Not inherently. Both achieve ±3 mmHg accuracy under the right conditions. Manual monitors are more accurate in trained hands, especially for patients with arrhythmias or circulation issues. Digital monitors are more consistent across different users, making them the better choice for home use and routine screening.
Which blood pressure monitor is best for home use? A validated digital upper-arm monitor is best for home use. They require no training, eliminate technique errors, and provide consistent readings. Look for devices with three-reading averaging and irregular heartbeat detection. Manual monitors are an option only if the user has clinical training.
Can digital blood pressure monitors be inaccurate? Yes, in certain cases. Digital monitors use oscillometric algorithms that can struggle with irregular heart rhythms, severe obesity, advanced arteriosclerosis, or weak pulse signals. In these situations, a trained clinician using a manual aneroid device will typically produce a more reliable reading.
What is the difference between aneroid and digital blood pressure monitors? Aneroid (manual) monitors use a pressure gauge and stethoscope — the user listens for arterial sounds to determine pressure. Digital monitors automate this process using oscillometric sensors and a microprocessor. Aneroid devices require training; digital devices work with minimal instruction.
How often should blood pressure monitors be calibrated? Manual aneroid devices should be calibrated at least once per year, or after any significant drop or impact. Premium models like the Welch Allyn DS66 offer calibration warranties of up to 15 years. Digital monitors should be checked periodically against a validated reference device.
Does cuff size affect blood pressure accuracy? Yes — significantly. An undersized cuff can produce falsely elevated readings; an oversized cuff can produce falsely low ones. The error can exceed 5–10 mmHg, which is larger than the accuracy difference between most manual and digital devices. Always match cuff size to the patient's arm circumference.
What blood pressure monitor do doctors use? Most clinical settings use a combination: digital automated monitors for routine screening and workflow efficiency, and manual aneroid sphygmomanometers for confirmation, complex patients, or training. Professional-grade options include the Welch Allyn ProBP 2400 (digital) and the Welch Allyn DuraShock DS45 (manual).









Manual blood pressure monitors offer greater clinical precision; digital monitors offer speed and consistency. The right choice depends on your setting: trained clinicians often prefer manual (aneroid) devices for complex cases, while digital monitors suit home users and high-volume screening. Most clinical guidelines recommend using both, digital for routine measurement, manual for confirmation.
This guide breaks down accuracy, ease of use, cost, and the best devices for each setting so you can choose with confidence.
TL;DR
Quick Summary: Manual vs. Digital Blood Pressure Monitors
| Manual (Aneroid) | Digital | |
|
Accuracy |
±3 mmHg (operator-dependent) | ±3 mmHg (automated) |
|
Best for |
Clinical confirmation, EMS, training | Home use, screening, busy clinics |
|
Ease of use |
Requires training | Minimal training needed |
|
Power needed |
No | Yes (battery/charging) |
|
Cost |
Lower upfront | Higher upfront |
|
Irregular rhythms |
Better detection | Algorithm limitations |
Bottom line: Use digital for speed and consistency. Use manual when accuracy is critical or patient factors complicate automated readings.
How Manual Blood Pressure Measurement Works
Manual blood pressure monitors, also known as aneroid sphygmomanometers, use an inflatable cuff, pressure gauge, and the stethoscope to measure blood pressure through auscultation.
This method remains a clinical standard because it allows trained users to directly hear arterial sounds and control the measurement process.
Entry-level tools like the ADC Basic Aneroid Sphygmomanometer (450-776Z) provide a reliable starting point, featuring:
- A precision-calibrated manometer gauge
- Index and range markings to support proper cuff placement
- A compact, pocket-sized design for portability
For clinicians needing greater durability and long-term performance, the ADC Prosphyg ™ 760 Pocket Aneroid (401-760-11ABK) offers:
- ±3 mmHg accuracy across standard temperature ranges
- A 300 mmHg black enamel manometer built for daily use
- ADC’s Size Guide™ cuff system, helping prevent mis-cuffing errors
Together, these tools illustrate how manual monitors can scale from student use to professional clinical environments.
The Case for Aneroid Sphygmomanometers
Manual devices continue to be preferred in many healthcare environments for several reasons:
High Accuracy with Proper Technique
Manual monitors provide clinically validated accuracy (typically ±3 mmHg) when used correctly, especially in controlled clinical environments.
Durability and Long-Term Reliability
Professional-grade models such as the Welch Allyn DuraShock ™ DS45 (450-DS45.11) are engineered for long-term reliability, featuring:
- Certified accuracy of ±3 mmHg
- Gear-free DuraShock™ technology, helping maintain calibration longer than traditional designs
- 30-inch drop resistance, meeting AAMI shock standards
For clinics requiring flexibility across multiple patient types, the DS45 Multi-Cuff Kit (450-DS45MC) includes:
- Four FlexiPort® cuffs (child to large adult)
- Quick cuff changes with a single-point connection system
In high-demand environments, advanced options like the Welch Allyn Gold Series DS66 Trigger Aneroid with 4 Cuff Kit (450-5098-30) and Welch Allyn Tycos Gold Series DuraShock DS66 Hand Aneroid with Adult Cuff (FlexiPort) (450-5098.27) add:
- One-handed trigger deflation control for precision
- Jeweled movement mechanisms for extended instrument life
- Up to 15-year calibration warranties
These features make them ideal for high-volume clinics, family practic, and long-term clinical use.
No Power Required
Manual monitors operate without batteries or charging, making them ideal for:
- Mobile clinicians
- Emergency response
- Training environments
Greater Clinical Control
Clinicians can control inflation, deflation, and auscultation technique, especially important for complex or irregular readings.
The Case for Digital Blood Pressure Monitors
Digital blood pressure monitors automate the measurement process, providing fast and easy readings with minimal training required.
A leading example is the Welch Allyn ProBP ™ 2400 Digital Blood Pressure Device (100-2400), designed for modern clinical workflows.
This device combines automation with advanced diagnostic support, including:
- ±3 mmHg measurement accuracy
- Three-reading averaging mode to improve diagnostic reliability
- Irregular heartbeat detection for added clinician insight
- Microprocessor-controlled deflation, reducing user error
Measurement range:
- Systolic: 60-255 mmHg
- Diastolic: 30-200 mmHg
The ProBP 2400 supports a wide range of patient needs while delivering consistent, repeatable readings across users.
Ease of Use
Digital devices are simple to operate, making them ideal for:
- Home users managing hypertension
- Busy clinics with multiple staff members
- Screening environments
Consistent Measurement Technique
Automated inflation and deflation reduce user variability, improving consistency across readings.
Advanced Clinical Features
Modern digital monitors often include:
- Multi-reading averaging
- Irregular heartbeat detection
- Controlled deflation technology
These features help provide a more complete picture of patient cardiovascular health.
Improved Workflow Efficiency
Digital devices support faster patient throughput, making them valuable in high-volume settings.
Accuracy Comparison: Manual vs. Digital Blood Pressure Monitors
Both device types can achieve clinically validated accuracy of ±3 mmHg — the benchmark set by AAMI standards — but how they get there differs significantly.
Manual (Aneroid) Monitors
Manual devices measure blood pressure through auscultation: a trained user listens for Korotkoff sounds while controlling cuff inflation and deflation. Accuracy depends heavily on the operator.
Strengths:
- ±3 mmHg accuracy when used by trained clinicians
- Less affected by irregular heart rhythms (atrial fibrillation, arrhythmias)
- Allows detection of subtle arterial sounds digital algorithms may miss
- No algorithmic interpretation — the clinician hears and decides
Limitations:
- Accuracy is operator-dependent; errors increase with less experienced users
- Requires proper cuff placement, controlled deflation rate, and quiet environment
- Not practical for self-measurement at home
When manual is the better choice: Patients with arrhythmias, severe obesity, advanced arteriosclerosis, diabetes affecting circulation, or weak pulse signals — situations where automated algorithms are more likely to produce unreliable readings.
Digital (Automated) Monitors
Digital monitors use oscillometric technology, detecting arterial wall vibrations rather than sound. A microprocessor interprets these oscillations to calculate systolic and diastolic pressure.
Strengths:
- ±3 mmHg accuracy; ±5% pulse accuracy (e.g., Welch Allyn ProBP 2400)
- Eliminates operator variability — same technique every time
- Three-reading averaging modes improve diagnostic reliability
- Irregular heartbeat detection flags readings that may need follow-up
- Faster workflow in high-volume settings
Limitations:
- Algorithms may underperform in certain patient populations
- Requires power source (batteries or charging)
- Higher upfront cost
When digital is the better choice: Routine screening, home monitoring, high-volume clinics, or any setting where consistent technique across multiple users matters more than nuanced clinical control.
Head-to-Head: The Honest Answer
Neither device type is universally superior. Clinical best practice — supported by major cardiovascular health organizations — increasingly recommends a combined approach:
- Digital for initial screening and routine monitoring
- Manual for confirmation when readings are abnormal, borderline, or the patient has factors that reduce digital accuracy
Regardless of device type, cuff fit remains the single biggest accuracy variable. An incorrectly sized cuff can shift readings by 5–10 mmHg, more than the difference between most comparable devices.
What the Research Says
Clinical evidence supports using both device types strategically:
- The American Heart Association (AHA) recommends upper-arm automated devices for home blood pressure monitoring, noting they reduce measurement error compared to manual technique in unsupervised settings.
- A 2019 review in Hypertension found that automated office blood pressure measurement (AOBP) produces readings closer to ambulatory blood pressure than traditional manual auscultation, due to the elimination of white-coat effect during attended measurement.
- AAMI/ISO standards (the benchmark for device certification) require blood pressure monitors to achieve a mean error of ≤5 mmHg with a standard deviation ≤8 mmHg, both manual and digital devices in this guide meet or exceed that threshold.
- Studies consistently show that cuff sizing errors account for a larger share of measurement inaccuracy than device type, underscoring the importance of proper fit regardless of which monitor you choose.
Sources: American Heart Association, Hypertension (AHA Journal), Association for the Advancement of Medical Instrumentation (AAMI)
Cost, Maintenance, and Longevity
Manual Monitors
- Lower upfront cost
- Minimal maintenance
- Long lifespan
- Occasional calibration checks required
Digital Monitors
- Higher initial investment
- Require batteries or charging
- More components that may require servicing
In high-use environments, manual monitors are often more cost-effective long-term.
Choosing the Right Blood Pressure Monitor for Your Setting
The best blood pressure monitor depends on where it’s being used and who is using it.
Different settings prioritize different things —accuracy, speed, ease of use, or portability.
Use the guide below to quickly find the right fit.
Clinical Settings (Clinics, Hospitals, Outpatient Care)
Best for: Accuracy + efficiency in high-volume environments
What matters most:
- Fast patient throughput
- Consistent readings across staff
- Ability to confirm results when needed
Recommended Setup:
- Digital for screening + manual for confirmation
Top Picks:
- Manual: Welch Allyn DuraShock DS45
- Multi-patient use: Welch Allyn DS45 Multi-Cuff Kit
- Advanced control: Welch Allyn DS66 Trigger Aneroid
Why this works:
- Digital improves workflow speed
- Manual ensures clinical accuracy when readings are uncertain
Home Use (Patients & Caregivers)
Best for: Simplicity + consistency
What matters most:
- Easy operation
- Reliable readings without training
- Clear, repeatable results
Top Picks:
- Easy, automated: Welch Allyn ProBP 2400 Digital Blood Pressure Device
- Budget manual option: ADC Basic Aneroid Sphygmomanometer
Why this works:
- Digital devices remove user error
- Manual devices are viable if the user has training
EMS & Mobile Care (Field Use, Home Visits, First Responders)
Best for: Reliability + portability
What matters most:
- No reliance on power or batteries
- Durability in unpredictable environments
- Fast, dependable readings
Top Picks:
- Portable professional: ADC Prosphyg 760 Pocket Aneroid
- Premium durability: Welch Allyn Gold Series DS66 Hand Aneroid
Why this works:
- Manual devices function anywhere
- Compact designed fit mobile workflows
Training & Education (Students & Clinical Training Programs)
Best for: Skill development + foundational learning
What matters most:
- Learning proper technique
- Understanding auscultation
- Building clinical confidence
Top Picks:
- Beginner-friendly: ADC Basic Aneroid Sphygmomanometer
- Step-up option: ADC Prosphyg 760 Pocket Aneroid
Why this works:
- Manual devices teach core clinical skills
- Builds a foundation before using digital tools
Quick Decision Guide
| Setting | Best Choice |
|
Clinical |
Digital + Manual |
|
Home |
Digital |
|
EMS / Mobile |
Manual |
|
Training |
Manual |
Why Cuff Size Matters More Than the Device
Choosing the right monitor is important, but cuff size has an even greater impact on accuracy.
Incorrect cuff sizing can lead to:
- Too small → falsely high readings
- Too large → falsely low readings
Multi-cuff systems such as the Welch Allyn DS45 Multi-Cuff Kit (450-DS45MC) ensure accurate readings across a wide range of patients, especially in clinical settings.
Final Thoughts
Manual and digital blood pressure monitors are not competing tools, they are complementary.
- Manual devices provide precision and control
- Digital devices offer speed and consistency
The best choice ultimately depends on your environment, experience level, and clinical needs.
Frequently Asked Questions
Are manual blood pressure monitors more accurate than digital? Not inherently. Both achieve ±3 mmHg accuracy under the right conditions. Manual monitors are more accurate in trained hands, especially for patients with arrhythmias or circulation issues. Digital monitors are more consistent across different users, making them the better choice for home use and routine screening.
Which blood pressure monitor is best for home use? A validated digital upper-arm monitor is best for home use. They require no training, eliminate technique errors, and provide consistent readings. Look for devices with three-reading averaging and irregular heartbeat detection. Manual monitors are an option only if the user has clinical training.
Can digital blood pressure monitors be inaccurate? Yes, in certain cases. Digital monitors use oscillometric algorithms that can struggle with irregular heart rhythms, severe obesity, advanced arteriosclerosis, or weak pulse signals. In these situations, a trained clinician using a manual aneroid device will typically produce a more reliable reading.
What is the difference between aneroid and digital blood pressure monitors? Aneroid (manual) monitors use a pressure gauge and stethoscope — the user listens for arterial sounds to determine pressure. Digital monitors automate this process using oscillometric sensors and a microprocessor. Aneroid devices require training; digital devices work with minimal instruction.
How often should blood pressure monitors be calibrated? Manual aneroid devices should be calibrated at least once per year, or after any significant drop or impact. Premium models like the Welch Allyn DS66 offer calibration warranties of up to 15 years. Digital monitors should be checked periodically against a validated reference device.
Does cuff size affect blood pressure accuracy? Yes — significantly. An undersized cuff can produce falsely elevated readings; an oversized cuff can produce falsely low ones. The error can exceed 5–10 mmHg, which is larger than the accuracy difference between most manual and digital devices. Always match cuff size to the patient's arm circumference.
What blood pressure monitor do doctors use? Most clinical settings use a combination: digital automated monitors for routine screening and workflow efficiency, and manual aneroid sphygmomanometers for confirmation, complex patients, or training. Professional-grade options include the Welch Allyn ProBP 2400 (digital) and the Welch Allyn DuraShock DS45 (manual).
